
https://absoluteprohibition.wordpress.com/2016/03/21/anne-laure-donskoy-on-workfare-coercion-in-uk/
di Anne-Laure Donskoy
Anne-Laure Donskoy_Survivor researcher, UK
While there is a lot of focus on coercion organised and implemented
in psychiatry, less attention is being paid to state engineered welfare
measures based on libertarian paternalism1, which have
coercive practices at their core. Among them are policies that strongly
support behavioural change using positive psychology and cognitive
behavioural therapy. Freidli and Stearn (2015)2 call this
“psychocompulsion”. These policies and measures are increasingly used to
ambush and coerce persons with disabilities and the long term sick into
adopting new ways of being and living conditions under the constant
threat of sanctions and which have driven many to attempt to their
lives. This paper builds on the work of Friedli and Stearn3 as
an attempt to highlight current coercive welfare policies, including
forcing ‘therapy’ on individuals, as human rights violation of the CRPD.
Background: Psychocompulsion as state sponsored human rights violations
Psychocompulsion, the use of psychological strategies to “nudge”
individuals to make “life changes” that fit a political ideology or
programme, is not entirely new to the UK. Already in the 1970s, some
long term job claimants would be sent for a medical examination, on the
premise that if people were not physically ill then they should be able
to find and take up work, any work. This had all the flavours of
Victorian paternalism written all over it. The ‘mentally disordered’ and
the ‘mentally handicapped’ experienced a particular brand of
paternalism, hidden away from society and from consciousness in
specialist homes and services, often suffering physical and mental abuse
or used in rehabilitation work with little or no protection.
Today, psychocompulsion in the UK has been promoted by the
Behavioural Insights Team (nicknamed the “Nudge Unit”), now in private
hands as a social purpose company but still working closely with the Cabinet Office4,
thereby guaranteeing prime influence on policy making. It is clear that
psychocompulsion is being used to lock individuals, including the long
term unemployed, the sick and persons with disabilities, into
back-to-work schemes as a conditionality of welfare. In recent months
and weeks, voices of dissent have arisen mostly from social movements,
denouncing the use of coercion which put people’s lives at risk5.
As Friedli and Stearn’s paper show, this finger wagging attitude has taken on a far more sinister slant.
First, it turns on its head the idea that unemployment is the product
of a failing economy by strongly suggesting that it is a state of mind,
worse still a ‘mental illness’ that can be corrected by changing the
psychology of claimants, thus placing the onus of responsibility for
success, for betterment, for choice etc. on the individuals themselves.
This totally ignores issues of social (in-)justice.
Second, it widens the scope by netting in the most vulnerable people
in society, specifically the long term sick and those with disabilities,
including psychosocial disabilities. This strategy narrowly avoids
attracting full-on accusations of discrimination by putting these
individuals on par with the long term unemployed and by stressing ad
nauseam that the policy is about helping people which should be
achieved through (any type of paid) employment. Paid employment becomes
the embodiment and the “pinnacle of human experience”.6
Third, the underlying premise that ‘work is good for you’ ignores
those dissenting voices which argue that without strong provisos (taking
into account the complexity of individual circumstances, choice,
timeliness, appropriateness as much as the quality of support and work
on offer) the argument is both unhelpful and counterproductive7, and can have devastating consequences for those concerned.
Finally, the stance of the policy totally fits within the libertarian
paternalism agenda which moves away from collective to total individual
(libertarian) responsibility, slowly realising Ayn Rand’s vision for a
permanently productive (and permanently disposable/replaceable)
workforce serving an elite. In this scheme, all coercive strategies
acquire a legitimacy that the psychiatric survivor movement rejects.
Being ill or disabled, and on welfare benefits: state coercion and the CRPD
The Welfare Reform Act 2012 introduced a wide range of reforms to the
benefits and tax credits system. The stated aim was to reduce the
financial burden of the cost of welfare. This is being achieved by
introducing ever drastic and punitive policies under the guises of a
responsibilisation agenda, underpinned with an intense authoritarian
ideology not seen or experienced since Victorian times. The Tory
manifesto of the 2015 general elections claimed it aimed to help people
with mental health issues back in to work. The reality is very
different and people with mental health issues clearly face
discriminations which other groups do not.
Article 4: The rights and freedoms of persons with disabilities are violated under the social security scrutiny regime:
When people with mental health issues are on welfare benefits, they
find themselves the object of intense, intrusive and inappropriate
scrutiny by the system, notably through the Work Capability Assessment
(WCA) which has consistently failed these claimants as it is totally
unsuited to their singular predicaments and experiences. As a result,
more and more people are placed on the Work Related Activity Group of
the Employment and Support Allowance which comes with strict
conditionalities. Also affected are those under the new Universal Credit
(UC) system which is being rolled out for all benefits claimants which
places yet another layer of scrutiny on individuals, possibly more so
those in work.
Article 1-5: Discrimination
A judicial review in 2013 found that the WCA process actively
discriminates against people with mental health issues. Since then very
little has been done to change the process and the status quo remains.
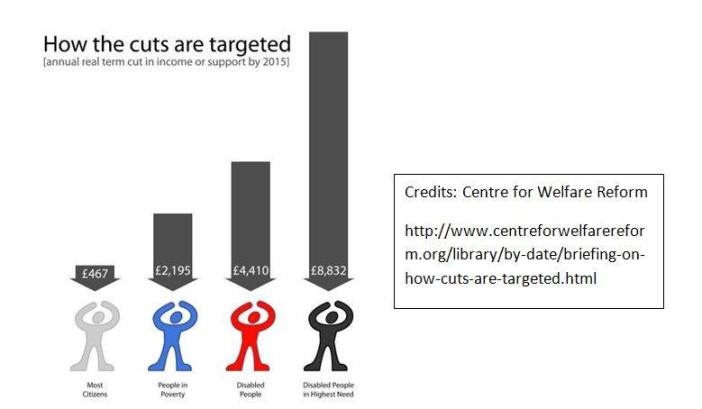
The Centre for Welfare reform, in its recent report A Fair Society?,
also shows that persons with disabilities are targeted the most despite
the fact that they have the greatest and often most complex needs.
Article 10: Right to life: “States Parties reaffirm
that every human being has the inherent right to life and shall take all
necessary measures to ensure its effective enjoyment by persons with
disabilities on an equal basis with others”.
A poll of over 1,000 GPs commissioned by Rethink Mental Illness in
2015, found that over 20% have patients who have felt suicidal due to
the WCA8.
In a report sent to the Department for Work and Pensions (DWP), the
senior coroner for inner north London, Mary Hassell, said “the trigger”
for the suicide was the man being found fit for work by the department”9.
[A Freedom of Information request has] revealed that the Department
for Work and Pensions (DWP) has investigated decisions, via peer
reviews, about the welfare payments of 60 claimants following their
deaths. A peer review, according to the DWP guidance for employees, must
be undertaken when suicide is associated with DWP activity to ensure
that any DWP action or involvement with the person was appropriate and
procedurally correct.10
Article 13: Access to justice: 13.1: “States Parties
shall ensure effective access to justice for persons with disabilities
on an equal basis with others, including through the provision of
procedural and age-appropriate accommodations, in order to facilitate
their effective role as direct and indirect participants, including as
witnesses, in all legal proceedings, including at investigative and
other preliminary stages.”
Benefit claimants who wish to appeal a decision need access to
justice. This represents an expense they can ill afford (if at all)
therefore need access to legal aid. However, the Ministry of Justice has
removed welfare benefits matters from the scope of legal aid funding,
thereby denying access to justice and discriminating against the most
vulnerable and poorest, among whom people with mental health issues:
In order to challenge a decision of a First-tier Tribunal (FtT) the
appellant needs to identify an error of law in the FtT’s decision and
then request permission to appeal to the Upper Tribunal (UT). The
process of appealing on a point of law to the UT has two stages, but,
for the reasons set out below, the legal aid contract only covers the
second stage … The absence of any legal aid at Stage One of an appeal to
a UT on a point of law represents a major flaw in the current scheme as
it is simply unrealistic to expect an appellant to draft an appeal on a
point of law without any assistance.11
In the future, social security claimants who find themselves faced
with an incorrect Upper Tribunal decision, or who win their case at the
Upper Tribunal but find themselves on the receiving end of an appeal by
the DWP12, HMRC13 or a local authority, could be facing the courts and the costs risks attached on their own or not at all.14
In practice, benefit claimants who wish to appeal decisions have to
resort to charitable organisations to support them through the process.
However these are seeing their funding cut, or they are not coping with
increasing number of calls for help.15 There has also been
some criticism from within the legal system with regard to persons with
intellectual disabilities on matters of legal representation regarding
privation of liberty; the same issues also apply to persons with
psychosocial disabilities:
The Law Society, which represents solicitors throughout England and
Wales, intervened [in a particular case]. Its president, Jonathan
Smithers, said: “When a vulnerable person doesn’t have friends or family
to represent them during a decision to restrict their liberty, it is
vital that person is able to participate in the decision-making process .
. . If this is not possible then they must have a legal representative
to protect their rights as well as their health and general welfare.
Those who are least able to defend themselves should not be sacrificed
on the altar of austerity.” 16
Actively changing the narrative of workfare and welfare benefits
The narrative of welfare is changing drastically. As Friedi says, we
are moving from a “what people have to do [to find work] to what they
have to be [demonstrating the right attitude to be employable]17. This is exemplified through the new ‘Work and Health Programme’ planned to be rolled out in England and Wales.
This programme has many strands, including:
− Embedding psychological services within Job Centres
− Placing ‘job coaches’ within GP surgeries for people with certain
conditions (specifically people with mental health issues): the
‘Working Better’ pilot scheme is funded by the Department for Work and
Pensions and the coaches will be provided by welfare to work agency,
Remploy (a welfare-to-work subsidiary of the Maximus).

This programme blurs the boundary between health and welfare, health
and work domains, in a way that has not happened before. This is a
coordinated move to effectively bring in the benefits system within NHS
care: joblessness, being unemployed becomes an illness, specifically a
mental illness which needs to and care be cured through psychological
therapies.
It will not only extend benefit conditionality into the NHS but also
compromise clinical independence and clinical ethics. In practice,
people who display the wrong attitude to work, to work
placements or who have been unemployed for a long time will be referred
to psychologists and given forced Cognitive Behavioural Therapy, and be
sent many motivational emails and text messages throughout the week; or
they will be prescribed referrals to an in-house ‘job coach’. Failure to
comply with these forced prescriptions will trigger an immediate
sanction regime. This will inevitably threaten if not destroy that first
quality that patients place in their doctor, trust. People may become
reluctant to say anything whether it is about their situation or their
health for fear of being forced into the schemes.
CRPD violations:
Articles 1-5: (equality, choice, autonomy, capacity)
Persons with disabilities are specifically targeted by the new measures
Article 25 (Right to health):
Currently both schemes are in the early stages of being rolled out
(pilot stage) and the official line claims that they are voluntary.
However, as the Tory manifesto stated “We will help you back into work
if you have a long-term yet treatable condition”, this is set to become
compulsory: “People who might benefit from treatment should get the
medical help they need so they can return to work. If they refuse a
recommended treatment, we will review whether their benefits should be
reduced.”(p. 28). However, being forced to receive “therapy” for a
“treatable condition” is not the same thing as being offered support,
which would imply that the individual is free to choose to take it up or
not. Most observers agree that what is currently taking place on a
voluntary basis as part of the pilot projects will become compulsory,
which would only follow the UK Government’s own stance of applying any
means to get people “back to work”18.
This means that people with mental health problems will no longer be
able to freely choose to consent, or withhold their consent, to
‘treatment’. There is also a high risk that people will feel intimidated
into consenting to undergo these ‘therapies’. This is very similar to
what happens in psychiatry whereby the right to health is invoked to
forcibly treat people for their own good, “in their best interest” … but
as their only option. To decline a recommended treatment or to fail to
comply to the letter with the injunctions and expectations of the system
will result in benefits sanctions.
Cognitive behavioural therapy (CBT), the approach chosen by the
Government is highly controversial and does not suit everybody.
Therefore a one-fits-all approach, whether it is applied forcibly or
not, will be counterproductive as it may make some people feel worse
(counter to their right to health) and shows the total lack of
understanding of the often complex and singular situations of persons
with disabilities.
Art 10: (Right to life)
Any Government that uses coercion and sanctions as a means to a
political end must take full responsibility for the consequences of its
actions. As with the Work Capability Assessment, people being coerced
into receiving behavioural or any therapy they did not fully consent to,
may experience adverse effects (making people even more unwell by
making them even poorer and forcing them to live in a constant state of
anxiety, making them suicidal).
It also denies the person as an autonomous individual able to make their own choices (Art 12, Equal recognition before the law; Art 16, Freedom from exploitation, violence and abuse and threatens their integrity (Art 17)).
It also contradicts the Government’s own claims that it is doing everything to make UK domestic law compliant with the CRPD:
The Convention is not legally binding in domestic law in the UK but
is given effect through the comprehensive range of existing and
developing legislation, policies and programmes that are collectively
delivering the Government’s vision of equality.19
Article 17 (Protecting the integrity of the person): The issue of coercion goes beyond “designating work as a cure for unemployment and poverty”20
as Friedli puts it; this is also about changing people’s societal
status and identity. In the new narrative, there are productive and
unproductive individuals, therefore there is no such thing as a
long-term sick or disabled person (all disabilities included). These
notions pretty much disappear in the name of inclusiveness and fairness
(in relation to so-called “hard working people”21 who are deserving of help and will do their utmost not to rely on the state for their individual needs).
Language is indeed important in this context, and language is
shifting. As many have observed, ‘sick notes’ have become ‘fit notes’,
the term ‘disability’ too is being erased as ‘Disability Living
Allowance’ becomes ‘Personal Individual Payment’. This speaks to a
simplistic but powerful narrative of ‘can-do-no-matter-what’ supported
by having a compulsory ‘right attitude, which is where psychocompulsion
comes in. Nudging then forcing people into having the ‘right attitude’.
Forcing people back to work by reducing their welfare benefits
Persons with disabilities are clearly targeted over and above other categories of individuals (Art 1-5 equality,
discrimination, choice, autonomy). Indeed, another form of coercion has
emerged through a recent drastic to the ESA in weekly support from £103
to £73, contained in the Welfare Reform and Work Bill. It will apply to
new ESA claimants in the work-related activity group. This vote, pushed
through Parliament on 7 March 201622, is meant to
“incentivise disabled people to find work quicker”. This (purely
ideological) decision will not only strip them of financial security but
also reinforce the idea, by bringing the rate into line with
Jobseeker’s Allowance, that disability no longer exists, that anyone can
and should work, that there are only productive (deserving) and
unproductive (undeserving) people.
An unethical social experiment
It has come to light that these new programmes are also the subject
of ‘research’. The new Work and Health Programme is currently at a
research and trialing stage23. As Kitty Jones writes,
Part of the experimental nudge element of this research entails
enlisting GPs to “prescribe” job coaches, and to participate in
constructing “a health and work passport to collate employment and
health information.24
However, this ‘research’ (if one can call it so), has been heavily
criticised because it is not sanctioned according to the usual robust
ethical guidelines. Research that adheres to robust ethical guidelines
would absolutely seek not to cause harm to its participants, and would
seek their informed consent beforehand25. This is not the
case here where claimants are the participants are the involuntary and
‘unconsented’ participants of an experiment they know nothing about.
There are a wide range of legal and Human Rights implications
connected with experimentation and research trials conducted on social
groups and human subjects.26
A spokesperson for Disabled People Against Cuts (DPAC), talked of the
UN CRPD Committee’s visit to the UK and described the situation thus:
It means the UN will examine the vicious and punitive attacks on
disabled people’s independent living as well as the cuts which have seen
so many placed in inhuman circumstances and has led to unnecessary
deaths.27
Articles 1-5: discrimination against persons with disabilities who are targeted through this programme.
Article 9: right to communication: The existence of this experiment and the format of its conduct has not been communicated with the claimants (the participants).
Article 10 (Right to Life): when coercion brings
people to the brink of suicide or they succeed in killing themselves
(one court case at least has pronounced on the clear link between
benefits sanctions and reasons for suicide):
Research from the Black Triangle campaign group found more than 80 cases of suicide directly linked to billions of pounds in benefit cuts. John McArdle, co-founder of Black Triangle, said: “The Dept of Work and Pensions refuses to reveal the findings of their own peer reviews of suicides linked
to the sanctions so we will never know the truth in those cases. . . He
said the Work Capability Assessment regime applied to all sick and
disabled people, without adequate risk assessment ‘built into the
system’28
Mortality rates bring their own tales of woe:
[The government] published or, rather, was forced to after several
Freedom of Information requests – that show more than 80 people a month
are dying after being declared “fit for work”. These are complex figures
but early analysis points to two notable facts. First that
2,380 people died between December 2011 and February 2014 shortly
after being judged “fit for work” and rejected for the sickness and
disability benefit, Employment and Support Allowance (ESA). We also now
know that 7,200 claimants died after being awarded ESA and being placed
in the work-related activity group – by definition, people whom the
government had judged were able to “prepare” to get back to work.29
Articles 12, 17, 19: Coercive measures embedded in
all aspects of the Work and Health Programme and its various tools and
strategies run counter to the premise that the person is free and able
to make choices for themselves, and considerably threatens their right
to independent living when they are forced into poverty.
Nothing seems to shift the current UK Government’s assault on people
with disabilities or long term sickness, and on their human rights. Not
the many Freedom of Information requests which have revealed that the
DWP did look into the death of 60 benefits claimants but sat on the
findings; nor a Commons Select Committee inquiry into benefits sanctions
in April 2015, nor the visit by the UN CRPD committee at the request of
a disability group (DPAC) in the late autumn of 2015, nor a coroner’s
report clearly linking a claimant’s suicide to the stress caused by the
Work Capability Assessment. The UK is effectively engineering and
encouraging coercive and punitive policies that specifically target
people with disabilities and the long term sick, putting their lives and
their future at high risk. Many have observed that ‘austerity’ was only
ever an excuse to establish and implement ideological policies. This is
not about saving money in hard times; this is about the willful
annihilation of the disabled, either through language or deeds.
March 2016
Notes:
1https://kittysjones.wordpress.com/2015/11/28/the-goverments-reductive-positivistic-approach-to-social-research- is-a-nudge-back-to-the-nineteenth-century/– The idea that it is both possible and legitimate for governments, public and private institutions to affect and change the behaviours of citizens whilst also [controversially] “respecting freedom of choice.”
2 Friedli L, et al. Med Humanit 2015;41:40–47. doi:10.1136/medhum-2014-010622
3 See also this short film: https://vimeo.com/157125824
4 http://www.behaviouralinsights.co.uk/
5 http://www.disabilitynewsservice.com/coroners-ground-breaking-verdict-suicide-was-triggered-by-fit-for-work-test/
6Cole M. Sociology contra government? The contest for the meaning of unemployment in UK policy debates. Work Employment Soc 2008;22(1):27–43.
7 Even the Department of Work and Pensions (DWP) who are driving these policies, acknowledged in a 2006 study have put forth provisos that “account must be taken of the nature and quality of work and its social context” and that, for sick and disabled people, “there is little direct reference or linkage to scientific evidence on the physical or mental health benefits of (early) (return to) work for sick or disabled people.” 8https://www.gov.uk/government/publications/is-work-good-for-your-health-and-well-being
https://www.rethink.org/media-centre/2012/09/new-gp-survey-shows-government-welfare-test-is-pushing- vulnerable-people-to-the-brink
9 See note 3
10 https://www.wsws.org/en/articles/2015/02/05/welf-f05.html
11 https://gclaw.wordpress.com/2014/05/30/what-legal-aid-is-still-available-for-work-undertaken-on-welfare-benefits-post-laspo/
12 Department of Works and Pensions
13 Her Majesty’s Revenue and Customs
14 http://www.cpag.org.uk/content/legal-aid-reform-or-termination
15 http://www.theguardian.com/society/2014/feb/25/benefit-cuts-welfare-linked-mental-health
16 http://www.theguardian.com/society/2016/mar/10/judge-challenges-government-over-legal-representation-for-
vulnerable-people?CMP=share_btn_tw
17 https://www.youtube.com/watch?v=Dt-V0e0-ipY
18 A side point has been made by Friedli and others about the questionable ethics of those clinical psychologists who accept to take part in such initiatives and about the rapid expansion of the back-to-work industry.
19 Office for Disability Issues, UK Initial Report On the UN Convention on the Rights of Persons with Disabilities, May 2011,
www.odi.gov.uk/un-report
20 https://www.youtube.com/watch?v=Dt-V0e0-ipY
21 An expression used as a constant leitmotiv by the UK government.
22 Ministers claimed “financial privilege” to assert the Commons’ right to have the final say on budgetary measures
23 http://php.york.ac.uk/inst/spru/research/summs/esa.php
24 https://kittysjones.wordpress.com/2015/12/14/the-department-for-work-and-pensions-dont-know-what-their-ethical-and- safeguarding-guidelines-are-but-still-claim-they-have-some/
25 https://en.wikipedia.org/wiki/Ethical_research_in_social_science
26 See note 15
27 http://www.disabilitynewsservice.com/confirmed-un-is-investigating-uks-grave-violations-of-disabled-peoples-rights/
28http://www.mirror.co.uk/news/uk-news/more-80-suicide-cases-directly-5634404
29 http://www.theguardian.com/commentisfree/2015/aug/27/death-britains-benefits-system-fit-for-work-safety-net
Nessun commento:
Posta un commento